Lessons in Antisense
Lesson 8 – ASO Pharmacodynamic Principles (Part 1)
June 9, 2025 by Dr. Stan Crooke
Introduction
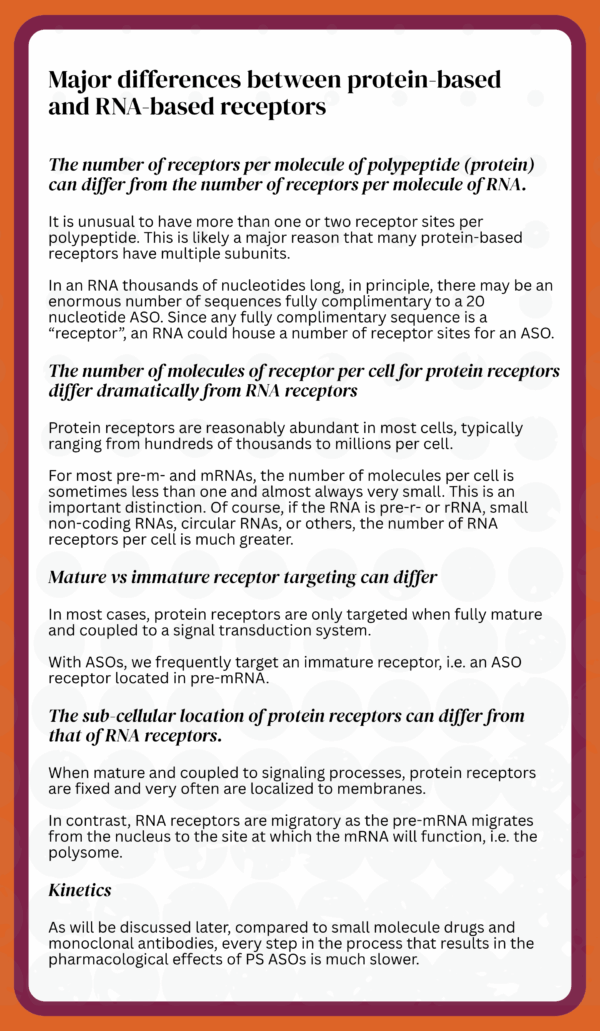
A critical first step in the evolution of ASO technology was the development of a theoretical framework within which to rationalize pharmacological observations. As receptor theory is the foundation on which the discipline of pharmacology rests, it made sense to adapt traditional receptor theory to rationalize the unique characteristics of ASOs. To do that, two concepts were essential. First, consider RNAs as a series of potential receptors for ASOs. Since ASOs are usually 18-20 nucleotides in length, a pre-mRNA or mRNA could be considered to have millions of potential receptor sites. Second, to consider ASOs as agents that alter the intermediary metabolism of RNA.
The pharmacological effects of all drugs, including ASOs, can be rationalized as occurring in three phases: Pre-receptor binding, receptor binding, and post-receptor binding. During the pre-receptor binding phase, it is sensible to think of the drug “sampling biological space to identify its cognate binding site or receptor”. In fact, the drug is binding to many biological sites, dissociating and binding to progressively higher affinity sites. In short, the drug is “traveling up its affinity curve” seeking the highest affinity site, the receptor. For most drugs, this phase is quite rapid. In the second phase, the drug binds to its receptor. Once again, for most drugs, this is an extremely rapid process. In the third phase, the post-receptor binding phase, the binding of the drug initiates a biological response often thought of as signal transduction. This process not only leads to biological effects but amplifies the effect of the drug because most receptors are directly coupled to signal transduction. Signal transduction is usually rapid and self-limited.
Though the basic principles of receptor theory can be adapted to rationalize the pharmacological effects of ASOs (including siRNAs), for almost every general principle, the behaviors of ASOs differ meaningfully from traditional small molecule drugs and monoclonal antibodies. I will try to highlight the differences.
Caveat: Because of the convenience of measuring target RNA reduction, most of the basic principles have derived from the study of PS ASOs that form duplexes cleaved by RNase H1. However, when we studied ASOs designed to work via other types of post-binding mechanisms, we observed behavior consistent with the principles established with RNase H1 ASOs.
It is likely that there is little to no free PS ASO in cells
Though we have not measured free PS ASO in cells, given the extensive protein and nucleic acid binding of PS ASOs, it is likely that there is no free PS ASO in cells at pharmacological doses.
Consequently, the concentration of PS ASO at sites in cells is the product of the Kds for binding sites and the concentration of those sites.
It also seems likely that when PS ASOs ultimately bind to their cognate RNA sequences (receptors), this step involves the transfer of PS ASO from a protein or a partially matched RNA sequence.
An important unanswered question is whether it is possible to saturate all PS ASO binding sites in the cell, resulting in free PS ASO. If so, that could play a factor at toxicological doses (I consider it unlikely that there is free PS ASO even at super toxic doses).
Mitochondria are “pharmacological hideouts”
We have never observed PS ASOs accumulating appreciable concentrations in mitochondria.
Nor have we observed any PS ASO activity in mitochondria.
PS ASOs can target all types of RNA in the cell
The more structured an RNA, the fewer sites are accessible to PS ASOs (and RNase H1).
Despite being highly structured and heavily modified, we have shown that PS ASOs can target pre-r or rRNAs, small molecular weight RNAs, and tRNAs (we never published tRNA data).
Circular, long non-coding and micro-RNAs are easily targeted by PS ASOs.
PS ASOs can produce pharmacological effects at sites throughout the cell (with the exception of mitochondria)
We have shown PS ASO activity in the nucleus, nucleolus, paraspeckles, spliceosomes, and during transcription.
In the cytoplasm, we have shown activity in the polysome and cytosol.
When corrected for volume, the potency of RNase H1 activating PS ASOs in the cytoplasm is about the same as in the nucleus.
Conclusions
ASOs are pharmacological agents, i.e., chemicals designed to produce a desired effect in humans. Consequently, a key step in creating and advancing ASO technology was to rationalize the technology in the context of pharmacological theory and ASOs are similar to traditional small molecule drugs, but differ in important ways. Most drugs are designed to treat or prevent disease, not “cure”. Today, it is possible to cure most infectious diseases and some cancers with drug therapy, but most chronic diseases require continuous treatment to correct or prevent the processes that lead to diseases and organ dysfunction. Dosing intervals are designed to replace the drug that is metabolized and cleared from the body so that a steady level of drug effect is produced.
Similar to small molecule drugs, ASOs are designed to bind to target sites, and we think of those sites as “receptors” for ASOs. Receptor theory teaches that, to be potent, a drug must interact effectively with its receptors in the body. Since the body presents an infinite array of sites to which a drug may bind, the most critical parameter to understand for any drug is its selectivity for binding to the desired target and not to other sites in the body. As a general rule, the more selective a drug is for binding to its receptor, the more precise the drug’s effects. Thus, drug discovery is primarily an effort to identify chemicals that can interact selectively with the desired receptors, and the more selective a drug is, the better its therapeutic index.
The therapeutic index of a drug is the single most important parameter to know about a drug. The most common way to calculate therapeutic index is to divide the potency for producing the desired effect vs undesired effects. Because the mid-point of any curve is the most accurate part of the curve, we typically divide the dose that produces 50% of the maximum desired effect into the dose that produces half-maximal adverse effects. The greater the therapeutic index, the better the drug.
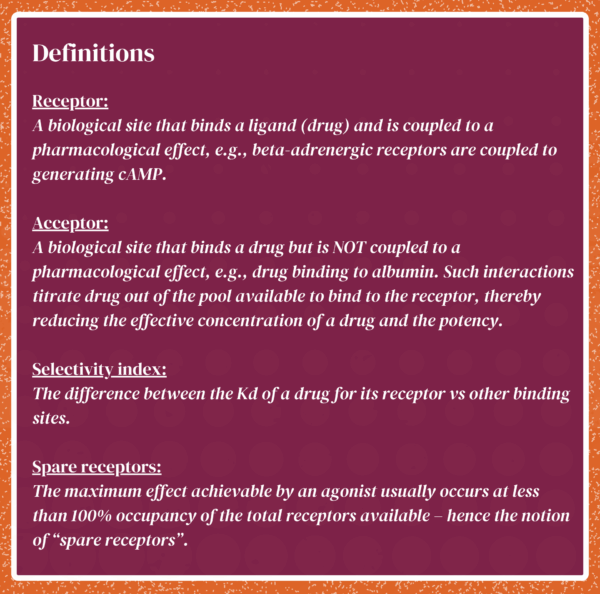
A receptor for a drug is a site to which the drug binds that is coupled to a biological response that amplifies the effects of the drug. Consequently, proteins like serum albumin are considered drug acceptors since albumin binds to many drugs but is not coupled to biological response. Receptor theory was developed for small molecule drug binding to proteins. The concept is generic.
“Receptors” for ASOs are complimentary sequences in RNAs and we take direct advantage of the genetic code to design ASOs that are extraordinarily specific for the target sequence in the target RNA. In contrast to traditional receptors that are usually coupled directly to a biological response, ASOs alter the production or abundance of an RNA or the maturation of an RNA to its final functional form.
One of the strengths of ASO technology is that ASOs can be designed to bind to any type of RNA and to cause RNAs to be degraded, or their processing to be altered, or ASOs can be used to block functions of RNAs, such as translation of an mRNA into a protein. Being able to design ASOs to do a variety of tasks after binding to a target RNA makes the technology quite versatile.


We cannot do
this alone
Together we are changing the world—
one patient at a time
We hope that you join us on this journey to discover, develop and provide individualized antisense medicines for free for life for nano-rare patients. The ultimate personalized medicine approach – for free, for life.

Follow us on social for updates on our latest efforts